
{kind=link}
{kind=link}
Bite size
Breaking down the challenge of inner-city childhood obesity
Read more

Note: Impact on Urban Health is part of Guy’s and St Thomas’ Foundation.
We take a programmatic approach to complex urban health issues, testing and exploring ideas with others. The content of this submission relates to insights from this approach. Our submission is forward looking, focusing on the priorities for further action in the UK.
Our current programmes address two issues:
These issues are prevalent in urban environments, complex in nature, and of interest beyond our boroughs. We aim to scale the impact of these programmes by sharing learning nationally and internationally. We collaborate with those who have the best approaches and share our drive to make them happen, from grassroot community groups to businesses. Whenever possible, we fund jointly with others.
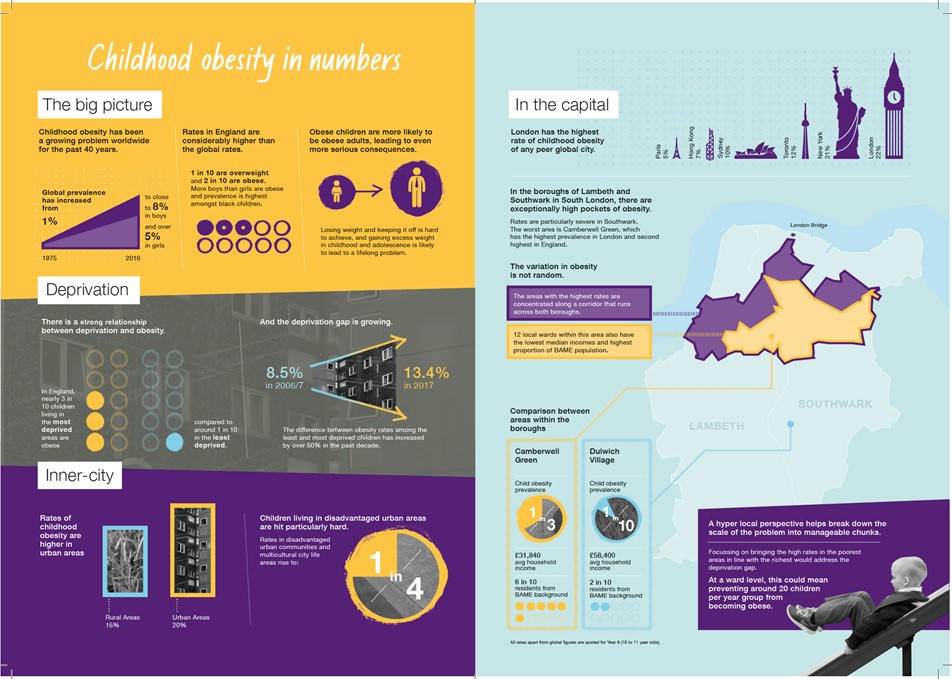
We focus on childhood obesity because London has the highest rates of any major global city, because it disproportionately affects the most disadvantaged communities, and because its effects play out over a lifetime. See Annex A: child obesity in numbers for further details.
We plan to tackle childhood obesity by taking a whole system, cross sector approach that focuses on creating environments that support and encourage nutritious eating and physical activity in places that children of all ages spend their time: home, school and streets.
Our children’s health and food programme will run for 10 years, during this time we plan to:
See here for further information on our children’s health and food programme model
In February 2018 we published a new report which explores childhood obesity in inner-city environments. It takes a detailed look at the evidence on behaviour change relating to deprived, urban and diverse environments.
On deprivation, we found that the relationship between income and childhood obesity is complex and influenced by factors beyond money itself. This complexity has implications for tackling the problem. For example, financial constraints may limit the effectiveness of promoting healthier but costlier foods. Likewise, encouraging parents to plan meals in advance and take the time to prepare fresh meals could be hampered by a lack of time and cognitive bandwidth.
Interventions that do not require individual action but are rather applied across the board, or are easy to take up, are likely to reduce health inequalities. This means prioritising “upstream” interventions, such as price promotion in shops at the point of purchase over “downstream” interventions like in-person dietary advice. Above all, it’s critical that policies do not rely heavily on resources that people may not have. Minimising the time, effort and costs of improving the diet and exercise of children is not only more likely to be effective, it is also less likely to increase health inequalities.
On urban settings we found that the built environment is a factor in driving the behaviours which lead to the development of childhood obesity. Many of these factors are exacerbated in urban areas. Perception of the environment also plays a part in influencing health-related behaviours.
When it comes to tackling the problem, these conclusions present both challenges and opportunities. On the one hand changing the physical environment is difficult and costly. Changes to planning regulations to reduce the density of fast food outlets are a legislative challenge, while building supportive facilities such as parks and cycle lanes is expensive. On the other, we have an opportunity: by changing perceptions about the environment we may be able to change how it influences behaviour. An example of this is reframing a commute as an opportunity for exercise. “Walk in to work out” was the slogan used in a randomised controlled trial in workplaces in Glasgow. Those that received a pack of interactive materials reframing commuting as an opportunity for exercise were twice as likely to increase walking compared to the control group.
On diversity we found that while there are consistent differences in childhood obesity rates across ethnicities, evidence suggests these are primarily due to environment rather than culturally specific behaviours.
As a result, ethnic and cultural practice might best be seen as an opportunity to take account of the communities in which children live, since this may allow for more effective interventions. For example, in some communities childhood obesity interventions recruiting children via places of religious worship have greater response rates compared to recruitment made through schools.
Research suggests that improving environments is the best route to creating long-term sustainable impact on childhood obesity. This in turn suggests the emphasis of effort should be on practical coordinated programmes, moving away from targeting specific individuals to initiatives that target whole populations within deprived areas.
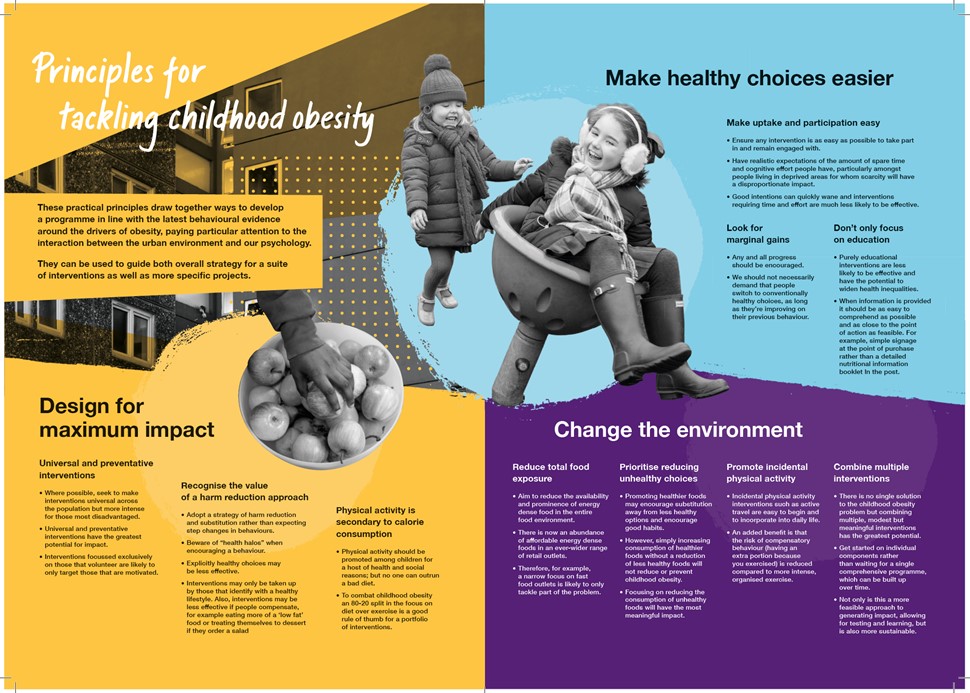
Working with the Behavioural Insights Team, practitioners in the field, our own projects with local communities, and drawing on evidence from national and international literature, we have developed a set of evidence based practical principles that government can use to inform priorities for further action:
See Annex B: principles for tackling childhood obesity for greater detail on the above.

Our response to the Mayor of London's office
How the environment influences what families eat
Our response to the Department for Environment, Food and Rural Affairs